
Asthma (from the Greek ἅσθμα, ásthma, "panting") is a common chronic inflammatory disease of the airways characterized by variable and recurring symptoms, reversible airflow obstruction, and bronchospasm. Common symptoms include wheezing, coughing, chest tightness, and shortness of breath.
Asthma is thought to be caused by a combination of genetic and environmental factors. Its diagnosis is usually based on the pattern of symptoms, response to therapy over time, and spirometry.
It is clinically classified according to the frequency of symptoms, forced expiratory volume in one second (FEV1), and peak expiratory flow rate.
Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic)[7] where atopy refers to a predisposition toward developing type 1 hypersensitivity reactions.
Treatment of acute symptoms is usually with an inhaled short-acting beta-2 agonist (such as salbutamol) and oral corticosteroids.
In very severe cases, intravenous corticosteroids, magnesium sulfate, and hospitalization may be required.
Symptoms can be prevented by avoiding triggers, such as allergens[11] and irritants, and by the use of inhaled corticosteroids.
Long-acting beta agonists (LABA) or leukotriene antagonists may be used in addition to inhaled corticosteroids if asthma symptoms remain uncontrolled.
The prevalence of asthma has increased significantly since the 1970s. In 2011, 235–300 million people globally have been diagnosed with asthma, and it caused 250,000 deaths.
Asthma is associated with exposure to indoor allergens.[36] Common indoor allergens include: dust mites, cockroaches, animal dander, and mold.[37][38] Efforts to decrease dust mites have been found to be ineffective.[39] Certain viral respiratory infections, such as respiratory syncytial virus and rhinovirus,[40] may increase the risk of developing asthma when acquired as young children.[41] Certain other infections, however, may decrease the risk.[40]
Use of antibiotics in early life has been linked to the development of asthma.[45] Also, delivery via caesarean section is associated with an increased risk (estimated at 20–80%) of asthma—this increased risk is attributed to the lack of healthy bacterial colonization that the newborn would have acquired from passage through the birth canal.[46][47] There is a link between asthma and the degree of affluence.[48]
Family history is a risk factor for asthma, with many different genes being implicated.[50] If one identical twin is affected, the probability of the other having the disease is approximately 25%.[50] By the end of 2005, 25 genes had been associated with asthma in six or more separate populations, including GSTM1, IL10, CTLA-4, SPINK5,LTC4S, IL4R and ADAM33, among others.[51]
Many of these genes are related to the immune system or modulating
inflammation. Even among this list of genes supported by highly
replicated studies, results have not been consistent among all
populations tested.[51] In 2006 over 100 genes were associated with asthma in one genetic association study alone;[51] more continue to be found.[52]
Some genetic variants may only cause asthma when they are combined with specific environmental exposures.[4] An example is a specific single nucleotide polymorphism in the CD14 region and exposure to endotoxin (a bacterial product). Endotoxin exposure can come from several environmental sources including tobacco smoke, dogs, and farms. Risk for asthma, then, is determined by both a person's genetics and the level of endotoxin exposure.[49]
There is a correlation between obesity and the risk of asthma with both having increased in recent years.[55][56] Several factors may be at play including decreased respiratory function due to a buildup of fat and the fact that adipose tissue leads to a pro-inflammatory state.[57]
Beta blocker medications such as propranolol can trigger asthma in those who are susceptible.[58] Cardioselective beta-blockers, however, appear safe in those with mild or moderate disease.[59] Other medications that can cause problems are ASA, NSAIDs, and angiotensin-converting enzyme inhibitors.[60]
Home factors that can lead to exacerbation of asthma include dust, animal dander (especially cat and dog hair), cockroach allergens and mold.[61] Perfumes are a common cause of acute attacks in women and children. Both viral and bacterial infections of the upper respiratory tract can worsen the disease.[61] Psychological stress may worsen symptoms—it is thought that stress alters the immune system and thus increases the airway inflammatory response to allergens and irritants.[31][62]

 Obstruction of the lumen of a bronchiole by mucoid exudate, goblet cell metaplasia, and epithelial basement membrane thickening in a person with asthma.
Asthma is the result of chronic inflammation of the airways which subsequently results in increased contractability of the surrounding smooth muscles.
This among other factors leads to bouts of narrowing of the airway and
the classic symptoms of wheezing. The narrowing is typically reversible
with or without treatment. Occasionally the airways themselves change.[16] Typical changes in the airways include an increase in eosinophils and thickening of the lamina reticularis.
Chronically the airways' smooth muscle may increase in size along with
an increase in the numbers of mucous glands. Other cell types involved
include: T lymphocytes, macrophages, and neutrophils. There may also be involvement of other components of the immune system including: cytokines, chemokines, histamine, and leukotrienes among others.[40]
Obstruction of the lumen of a bronchiole by mucoid exudate, goblet cell metaplasia, and epithelial basement membrane thickening in a person with asthma.
Asthma is the result of chronic inflammation of the airways which subsequently results in increased contractability of the surrounding smooth muscles.
This among other factors leads to bouts of narrowing of the airway and
the classic symptoms of wheezing. The narrowing is typically reversible
with or without treatment. Occasionally the airways themselves change.[16] Typical changes in the airways include an increase in eosinophils and thickening of the lamina reticularis.
Chronically the airways' smooth muscle may increase in size along with
an increase in the numbers of mucous glands. Other cell types involved
include: T lymphocytes, macrophages, and neutrophils. There may also be involvement of other components of the immune system including: cytokines, chemokines, histamine, and leukotrienes among others.[40]
There is currently no precise test with the diagnosis typically based on the pattern of symptoms and response to therapy over time.[5][40] A diagnosis of asthma should be suspected if there is a history of: recurrent wheezing, coughing or difficulty breathing and these symptoms occur or worsen due to exercise, viral infections, allergens or air pollution.[63] Spirometry is then used to confirm the diagnosis.[63] In children under the age of six the diagnosis is more difficult as they are too young for spirometry.[64]
Other supportive evidence includes: a ≥20% difference in peak expiratory flow rate on at least three days in a week for at least two weeks, a ≥20% improvement of peak flow following treatment with either salbutamol, inhaled corticosteroids or prednisone, or a ≥20% decrease in peak flow following exposure to a trigger.[69] Testing peak expiratory flow is more variable than spirometry, however, and thus not recommended for routine diagnosis. It may be useful for daily self-monitoring in those with moderate to severe disease and for checking the effectiveness of new medications. It may also be helpful in guiding treatment in those with acute exacerbations.[70]
Asthma is clinically classified according to the frequency of symptoms, forced expiratory volume in one second (FEV1), and peak expiratory flow rate.[6]
Asthma may also be classified as atopic (extrinsic) or non-atopic
(intrinsic), based on whether symptoms are precipitated by allergens
(atopic) or not (non-atopic).[7]
While asthma is classified based on severity, at the moment there is no
clear method for classifying different subgroups of asthma beyond this
system.[71]
Finding ways to identify subgroups that respond well to different types
of treatments is a current critical goal of asthma research.[71]
Although asthma is a chronic obstructive condition, it is not considered as a part of chronic obstructive pulmonary disease as this term refers specifically to combinations of disease that are irreversible such as bronchiectasis, chronic bronchitis, and emphysema.[72] Unlike these diseases, the airway obstruction in asthma is usually reversible; however, if left untreated, the chronic inflammation from asthma can lead the lungs to become irreversibly obstructed due to airway remodeling.[73] In contrast to emphysema, asthma affects the bronchi, not the alveoli.[74]
An acute asthma exacerbation is commonly referred to as an asthma attack. The classic symptoms are shortness of breath, wheezing, and chest tightness.[40] While these are the primary symptoms of asthma,[76] some people present primarily with coughing, and in severe cases, air motion may be significantly impaired such that no wheezing is heard.[75]
Signs which occur during an asthma attack include the use of accessory muscles of respiration (sternocleidomastoid and scalene muscles of the neck), there may be a paradoxical pulse (a pulse that is weaker during inhalation and stronger during exhalation), and over-inflation of the chest.[77] A blue color of the skin and nails may occur from lack of oxygen.[78]
In a mild exacerbation the peak expiratory flow rate (PEFR) is ≥200 L/min or ≥50% of the predicted best.[79] Moderate is defined as between 80 and 200 L/min or 25% and 50% of the predicted best while severe is defined as ≤ 80 L/min or ≤25% of the predicted best.[79]
Acute severe asthma, previously known as status asthmaticus, is an acute exacerbation of asthma that does not respond to standard treatments of bronchodilators and corticosteroids.[80] Half of cases are due to infections with others caused by allergen, air pollution, or insufficient or inappropriate medication use.[80]
Brittle asthma is a kind of asthma distinguishable by recurrent, severe attacks.[75] Type 1 brittle asthma is a disease with wide peak flow variability, despite intense medication. Type 2 brittle asthma is background well-controlled asthma with sudden severe exacerbations.[75]
Chronic obstructive pulmonary disease can coexist with asthma and can occur as a complication of chronic asthma. After the age of 65 most people with obstructive airway disease will have asthma and COPD. In this setting, COPD can be differentiated by increased airway neutrophils, abnormally increased wall thickness, and increased smooth muscle in the bronchi. However, this level of investigation is not performed due to COPD and asthma sharing similar principles of management: corticosteroids, long acting beta agonists, and smoking cessation.[90] It closely resembles asthma in symptoms, is correlated with more exposure to cigarette smoke, an older age, less symptom reversibility after bronchodilator administration, and decreased likelihood of family history of atopy.[91][92]
The most effective treatment for asthma is identifying triggers, such as cigarette smoke, pets, or aspirin, and eliminating exposure to them. If trigger avoidance is insufficient, the use of medication is recommended. Pharmaceutical drugs are selected based on, among other things, the severity of illness and the frequency of symptoms. Specific medications for asthma are broadly classified into fast-acting and long-acting categories.[99][100]
Bronchodilators are recommended for short-term relief of symptoms. In those with occasional attacks, no other medication is needed. If mild persistent disease is present (more than two attacks a week), low-dose inhaled corticosteroids or alternatively, an oral leukotriene antagonist or a mast cell stabilizer is recommended. For those who have daily attacks, a higher dose of inhaled corticosteroids is used. In a moderate or severe exacerbation, oral corticosteroids are added to these treatments.[9]
"Manual therapies", including osteopathic, chiropractic, physiotherapeutic and respiratory therapeutic maneuvers, have insufficient evidence to support their use in treating asthma.[132] The Buteyko breathing technique for controlling hyperventilation may result in a reduction in medications use however does not have any effect on lung function.[100] Thus an expert panel felt that evidence was insufficient to support its use.[129]
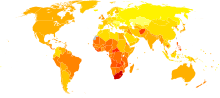
Disability-adjusted life year for asthma per 100,000 inhabitants in 2004.[133]
The prognosis for asthma is generally good, especially for children with mild disease.[134] Mortality has decreased over the last few decades due to better recognition and improvement in care.[135]
Globally it causes moderate or severe disability in 19.4 million people
as of 2004 (16 million of which are in low and middle income
countries).[136] Of asthma diagnosed during childhood, half of cases will no longer carry the diagnosis after a decade.[50] Airway remodeling is observed, but it is unknown whether these represent harmful or beneficial changes.[137] Early treatment with corticosteroids seems to prevent or ameliorates a decline in lung function.[138]

Rates of asthma in different countries of the world as of 2004.
As of 2011, 235–300 million people worldwide are affected by asthma,[14][15] and approximately 250,000 people die per year from the disease.[16] Rates vary between countries with prevalences between 1 and 18%.[16] It is more common in developed than developing countries.[16] One thus sees lower rates in Asia, Eastern Europe and Africa.[40]
Within developed countries it is more common in those who are
economically disadvantaged while in contrast in developing countries it
is more common in the affluent.[16] The reason for these differences is not well known.[16] Low and middle income countries make up more than 80% of the mortality.[139]
While asthma is twice as common in boys as girls,[16] severe asthma occurs at equal rates.[140] In contrast adult women have a higher rate of asthma than men[16] and it is more common in the young than the old.[40]
Global rates of asthma have increased significantly between the 1960s and 2008[141][142] with it being recognized as a major public health problem since the 1970s.[40] Rates of asthma have plateaued in the developed world since the mid-1990s with recent increases primarily in the developing world.[143] Asthma affects approximately 7% of the population of the United States[110] and 5% of people in the United Kingdom.[144] Canada, Australia and New Zealand have rates of about 14–15%.[145]

1907 advertisement for Grimault's Indian Cigarettes, emphasising their
alleged efficacy for the relief of asthma and other respiratory
conditions
Asthma was recognized in Ancient Egypt and was treated by drinking an incense mixture known as kyphi.[146] It was officially named as a specific respiratory problem by Hippocrates circa 450 BC, with the Greek word for "panting" forming the basis of our modern name.[40] In 200 BC it was believed to be at least partly related to the emotions.[23]
In 1873, one of the first papers in modern medicine on the subject tried to explain the pathophysiology of the disease while one in 1872, concluded that asthma can be cured by rubbing the chest with chloroform liniment.[147][148] Medical treatment in 1880, included the use of intravenous doses of a drug called pilocarpin.[149] In 1886, F.H. Bosworth theorized a connection between asthma and hay fever.[150] Epinephrine was first referred to in the treatment of asthma in 1905.[151] Oral corticosteroids began to be used for this condition in the 1950s while inhaled corticosteroids and selective short acting beta agonist came into wide use in the 1960s.[152][153]
During the 1930s–1950s, asthma was known as one of the "holy seven" psychosomatic illnesses. Its cause was considered to be psychological, with treatment often based on psychoanalysis and other talking cures.[154] As these psychoanalysts interpreted the asthmatic wheeze as the suppressed cry of the child for its mother, they considered the treatment of depression to be especially important for individuals with asthma.
SOURCE: wikipedia
Asthma is thought to be caused by a combination of genetic and environmental factors. Its diagnosis is usually based on the pattern of symptoms, response to therapy over time, and spirometry.
It is clinically classified according to the frequency of symptoms, forced expiratory volume in one second (FEV1), and peak expiratory flow rate.
Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic)[7] where atopy refers to a predisposition toward developing type 1 hypersensitivity reactions.
Treatment of acute symptoms is usually with an inhaled short-acting beta-2 agonist (such as salbutamol) and oral corticosteroids.
In very severe cases, intravenous corticosteroids, magnesium sulfate, and hospitalization may be required.
Symptoms can be prevented by avoiding triggers, such as allergens[11] and irritants, and by the use of inhaled corticosteroids.
Long-acting beta agonists (LABA) or leukotriene antagonists may be used in addition to inhaled corticosteroids if asthma symptoms remain uncontrolled.
The prevalence of asthma has increased significantly since the 1970s. In 2011, 235–300 million people globally have been diagnosed with asthma, and it caused 250,000 deaths.
Signs and symptoms
Asthma is characterized by recurrent episodes of wheezing, shortness of breath, chest tightness, and coughing.[16] Sputum may be produced from the lung by coughing but is often hard to bring up.[17] During recovery from an attack it may appear pus like due to high levels of white blood cells called eosinophils.[18] Symptoms are usually worse at night and in the early morning or in response to exercise or cold air.[19] Some people with asthma rarely experience symptoms, usually in response to triggers, whereas others may have marked and persistent symptoms.[20]Associated conditions
A number of other health conditions occur more frequently in those with asthma, including gastro-esophageal reflux disease (GERD), rhinosinusitis, and obstructive sleep apnea.[21] Psychological disorders are also more common,[22] with anxiety disorders occurring in between 16–52% and mood disorders in 14–41%.[23] However, it is not known if asthma causes psychological problems or if psychological problems lead to asthma.[24]Causes
Asthma is caused by a combination of complex and incompletely understood environmental and genetic interactions.[4][25] These factors influence both its severity and its responsiveness to treatment.[26] It is believed that the recent increased rates of asthma are due to changing epigenetics (heritable factors other than those related to the DNA sequence) and a changing living environment.[27]Environmental
Many environmental factors have been associated with asthma's development and exacerbation including allergens, air pollution, and other environmental chemicals.[28] Smoking during pregnancy and after delivery is associated with a greater risk of asthma-like symptoms.[29] Low air quality from factors such as traffic pollution or high ozone levels,[30] has been associated with both asthma development and increased asthma severity.[31] Exposure to indoor volatile organic compounds may be a trigger for asthma; formaldehyde exposure, for example, has a positive association.[32] Also, phthalates in PVC are associated with asthma in children and adults[33][34] as are high levels of endotoxin exposure.[35]Asthma is associated with exposure to indoor allergens.[36] Common indoor allergens include: dust mites, cockroaches, animal dander, and mold.[37][38] Efforts to decrease dust mites have been found to be ineffective.[39] Certain viral respiratory infections, such as respiratory syncytial virus and rhinovirus,[40] may increase the risk of developing asthma when acquired as young children.[41] Certain other infections, however, may decrease the risk.[40]
Hygiene hypothesis
The hygiene hypothesis is a theory which attempts to explain the increased rates of asthma worldwide as a direct and unintended result of reduced exposure, during childhood, to non-pathogenic bacteria and viruses.[42][43] It has been proposed that the reduced exposure to bacteria and viruses is due, in part, to increased cleanliness and decreased family size in modern societies.[44] Evidence supporting the hygiene hypothesis includes lower rates of asthma on farms and in households with pets.[44]Use of antibiotics in early life has been linked to the development of asthma.[45] Also, delivery via caesarean section is associated with an increased risk (estimated at 20–80%) of asthma—this increased risk is attributed to the lack of healthy bacterial colonization that the newborn would have acquired from passage through the birth canal.[46][47] There is a link between asthma and the degree of affluence.[48]
Genetic
| Endotoxin levels | CC genotype | TT genotype |
|---|---|---|
| High exposure | Low risk | High risk |
| Low exposure | High risk | Low risk |
Some genetic variants may only cause asthma when they are combined with specific environmental exposures.[4] An example is a specific single nucleotide polymorphism in the CD14 region and exposure to endotoxin (a bacterial product). Endotoxin exposure can come from several environmental sources including tobacco smoke, dogs, and farms. Risk for asthma, then, is determined by both a person's genetics and the level of endotoxin exposure.[49]
Medical conditions
A triad of atopic eczema, allergic rhinitis and asthma is called atopy.[53] The strongest risk factor for developing asthma is a history of atopic disease;[41] with asthma occurring at a much greater rate in those who have either eczema or hay fever.[54] Asthma has been associated with Churg–Strauss syndrome, an autoimmune disease and vasculitis. Individuals with certain types of urticaria may also experience symptoms of asthma.[53]There is a correlation between obesity and the risk of asthma with both having increased in recent years.[55][56] Several factors may be at play including decreased respiratory function due to a buildup of fat and the fact that adipose tissue leads to a pro-inflammatory state.[57]
Beta blocker medications such as propranolol can trigger asthma in those who are susceptible.[58] Cardioselective beta-blockers, however, appear safe in those with mild or moderate disease.[59] Other medications that can cause problems are ASA, NSAIDs, and angiotensin-converting enzyme inhibitors.[60]
Exacerbation
Some individuals will have stable asthma for weeks or months and then suddenly develop an episode of acute asthma. Different individuals react differently to various factors.[61] Most individuals can develop severe exacerbation from a number of triggering agents.[61]Home factors that can lead to exacerbation of asthma include dust, animal dander (especially cat and dog hair), cockroach allergens and mold.[61] Perfumes are a common cause of acute attacks in women and children. Both viral and bacterial infections of the upper respiratory tract can worsen the disease.[61] Psychological stress may worsen symptoms—it is thought that stress alters the immune system and thus increases the airway inflammatory response to allergens and irritants.[31][62]
Pathophysiology
Main article: Pathophysiology of asthma

Diagnosis
While asthma is a well recognized condition, there is not one universal agreed upon definition.[40] It is defined by the Global Initiative for Asthma as "a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyper-responsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness and coughing particularly at night or in the early morning. These episodes are usually associated with widespread but variable airflow obstruction within the lung that is often reversible either spontaneously or with treatment".[16]There is currently no precise test with the diagnosis typically based on the pattern of symptoms and response to therapy over time.[5][40] A diagnosis of asthma should be suspected if there is a history of: recurrent wheezing, coughing or difficulty breathing and these symptoms occur or worsen due to exercise, viral infections, allergens or air pollution.[63] Spirometry is then used to confirm the diagnosis.[63] In children under the age of six the diagnosis is more difficult as they are too young for spirometry.[64]
Spirometry
Spirometry is recommended to aid in diagnosis and management.[65][66] It is the single best test for asthma. If the FEV1 measured by this technique improves more than 12% following administration of a bronchodilator such as salbutamol, this is supportive of the diagnosis.[67] It however may be normal in those with a history of mild asthma, not currently acting up. Single-breath diffusing capacity can help differentiate asthma from COPD.[40] It is reasonable to perform spirometry every one or two years to follow how well a person's asthma is controlled.[68]Others
The methacholine challenge involves the inhalation of increasing concentrations of a substance that causes airway narrowing in those predisposed. If negative it means that a person does not have asthma; if positive, however, it is not specific for the disease.[40]Other supportive evidence includes: a ≥20% difference in peak expiratory flow rate on at least three days in a week for at least two weeks, a ≥20% improvement of peak flow following treatment with either salbutamol, inhaled corticosteroids or prednisone, or a ≥20% decrease in peak flow following exposure to a trigger.[69] Testing peak expiratory flow is more variable than spirometry, however, and thus not recommended for routine diagnosis. It may be useful for daily self-monitoring in those with moderate to severe disease and for checking the effectiveness of new medications. It may also be helpful in guiding treatment in those with acute exacerbations.[70]
Classification
| Severity | Symptom frequency | Night time symptoms | %FEV1 of predicted | FEV1 Variability | SABA use |
|---|---|---|---|---|---|
| Intermittent | ≤2/week | ≤2/month | ≥80% | <20 td=""> | ≤2 days/week |
| Mild persistent | >2/week | 3–4/month | ≥80% | 20–30% | >2 days/week |
| Moderate persistent | Daily | >1/week | 60–80% | >30% | daily |
| Severe persistent | Continuously | Frequent (7×/week) | <60 td=""> | >30% | ≥twice/day |
Although asthma is a chronic obstructive condition, it is not considered as a part of chronic obstructive pulmonary disease as this term refers specifically to combinations of disease that are irreversible such as bronchiectasis, chronic bronchitis, and emphysema.[72] Unlike these diseases, the airway obstruction in asthma is usually reversible; however, if left untreated, the chronic inflammation from asthma can lead the lungs to become irreversibly obstructed due to airway remodeling.[73] In contrast to emphysema, asthma affects the bronchi, not the alveoli.[74]
Asthma exacerbation
| Near-fatal | High PaCO2 and/or requiring mechanical ventilation | |
|---|---|---|
| Life threatening (any one of) |
||
| Clinical signs | Measurements | |
| Altered level of consciousness | Peak flow < 33% | |
| Exhaustion | Oxygen saturation < 92% | |
| Arrhythmia | PaO2 < 8 kPa | |
| Low blood pressure | "Normal" PaCO2 | |
| Cyanosis | ||
| Silent chest | ||
| Poor respiratory effort | ||
| Acute severe (any one of) |
||
| Peak flow 33–50% | ||
| Respiratory rate ≥ 25 breaths per minute | ||
| Heart rate ≥ 110 beats per minute | ||
| Unable to complete sentences in one breath | ||
| Moderate | Worsening symptoms | |
| Peak flow 50–80% best or predicted | ||
| No features of acute severe asthma | ||
Signs which occur during an asthma attack include the use of accessory muscles of respiration (sternocleidomastoid and scalene muscles of the neck), there may be a paradoxical pulse (a pulse that is weaker during inhalation and stronger during exhalation), and over-inflation of the chest.[77] A blue color of the skin and nails may occur from lack of oxygen.[78]
In a mild exacerbation the peak expiratory flow rate (PEFR) is ≥200 L/min or ≥50% of the predicted best.[79] Moderate is defined as between 80 and 200 L/min or 25% and 50% of the predicted best while severe is defined as ≤ 80 L/min or ≤25% of the predicted best.[79]
Acute severe asthma, previously known as status asthmaticus, is an acute exacerbation of asthma that does not respond to standard treatments of bronchodilators and corticosteroids.[80] Half of cases are due to infections with others caused by allergen, air pollution, or insufficient or inappropriate medication use.[80]
Brittle asthma is a kind of asthma distinguishable by recurrent, severe attacks.[75] Type 1 brittle asthma is a disease with wide peak flow variability, despite intense medication. Type 2 brittle asthma is background well-controlled asthma with sudden severe exacerbations.[75]
Exercise-induced
Main article: Exercise-induced bronchoconstriction
Exercise can trigger bronchoconstriction in both people with and without asthma.[81] It occurs in most people with asthma and up to 20% of people without asthma.[81] In athletes is diagnosed more commonly in elite athletes, with rates varying from 3% for bobsled racers to 50% for cycling and 60% for cross-country skiing.[81] While it may occur with any weather conditions it is more common when it is dry and cold.[82] Inhaled beta2-agonists do not appear to improve athletic performance among those without asthma[83] however oral doses may improve endurance and strength.[84][85]Occupational
Main article: Occupational asthma
Asthma as a result of (or worsened by) workplace exposures, is a commonly reported occupational disease.[86] Many cases however are not reported or recognized as such.[87][88]
It is estimated that 5–25% of asthma cases in adults are work–related. A
few hundred different agents have been implicated with the most common
being: isocyanates, grain and wood dust, colophony, soldering flux, latex, animals, and aldehydes. The employment associated with the highest risk of problems include: those who spray paint, bakers and those who process food, nurses, chemical workers, those who work with animals, welders, hairdressers and timber workers.[86]Differential diagnosis
Many other conditions can cause symptoms similar to those of asthma. In children, other upper airway diseases such as allergic rhinitis and sinusitis should be considered as well as other causes of airway obstruction including: foreign body aspiration, tracheal stenosis or laryngotracheomalacia, vascular rings, enlarged lymph nodes or neck masses. In adults, COPD, congestive heart failure, airway masses, as well as drug-induced coughing due to ACE inhibitors should be considered. In both populations vocal cord dysfunction may present similarly.[89]Chronic obstructive pulmonary disease can coexist with asthma and can occur as a complication of chronic asthma. After the age of 65 most people with obstructive airway disease will have asthma and COPD. In this setting, COPD can be differentiated by increased airway neutrophils, abnormally increased wall thickness, and increased smooth muscle in the bronchi. However, this level of investigation is not performed due to COPD and asthma sharing similar principles of management: corticosteroids, long acting beta agonists, and smoking cessation.[90] It closely resembles asthma in symptoms, is correlated with more exposure to cigarette smoke, an older age, less symptom reversibility after bronchodilator administration, and decreased likelihood of family history of atopy.[91][92]
Prevention
The evidence for the effectiveness of measures to prevent the development of asthma is weak.[93] Some show promise including: limiting smoke exposure both in utero and after delivery, breastfeeding, and increased exposure to daycare or large families but none are well supported enough to be recommended for this indication.[93] Early pet exposure may be useful.[94] Results from exposure to pets at other times are inconclusive[95] and it is only recommended that pets be removed from the home if a person has allergic symptoms to said pet.[96] Dietary restrictions during pregnancy or when breast feeding have not been found to be effective and thus are not recommended.[96] Reducing or eliminating compounds known to sensitive people from the work place may be effective.[86]Management
While there is no cure for asthma, symptoms can typically be improved.[97] A specific, customized plan for proactively monitoring and managing symptoms should be created. This plan should include the reduction of exposure to allergens, testing to assess the severity of symptoms, and the usage of medications. The treatment plan should be written down and advise adjustments to treament according to changes in symptoms.[98]The most effective treatment for asthma is identifying triggers, such as cigarette smoke, pets, or aspirin, and eliminating exposure to them. If trigger avoidance is insufficient, the use of medication is recommended. Pharmaceutical drugs are selected based on, among other things, the severity of illness and the frequency of symptoms. Specific medications for asthma are broadly classified into fast-acting and long-acting categories.[99][100]
Bronchodilators are recommended for short-term relief of symptoms. In those with occasional attacks, no other medication is needed. If mild persistent disease is present (more than two attacks a week), low-dose inhaled corticosteroids or alternatively, an oral leukotriene antagonist or a mast cell stabilizer is recommended. For those who have daily attacks, a higher dose of inhaled corticosteroids is used. In a moderate or severe exacerbation, oral corticosteroids are added to these treatments.[9]
Lifestyle modification
Avoidance of triggers is a key component of improving control and preventing attacks. The most common triggers include allergens, smoke (tobacco and other), air pollution, non selective beta-blockers, and sulfite-containing foods.[101][102] Cigarette smoking and second-hand smoke (passive smoke) may reduce the effectiveness of medications such as corticosteroids.[103] Dust mite control measures, including air filtration, chemicals to kill mites, vacuuming, mattress covers and others methods had no effect on asthma symptoms.[39] Overall exercise, however is beneficial in people with stable asthma.[104]Medications
Medications used to treat asthma are divided into two general classes: quick-relief medications used to treat acute symptoms; and long-term control medications used to prevent further exacerbation.[99]- Fast–acting

- Short-acting beta2-adrenoceptor agonists (SABA), such as salbutamol (albuterol USAN) are the first line treatment for asthma symptoms.[9]
- Anticholinergic medications, such as ipratropium bromide, provide additional benefit when used in combination with SABA in those with moderate or severe symptoms.[9] Anticholinergic bronchodilators can also be used if a person cannot tolerate a SABA.[72]
- Older, less selective adrenergic agonists, such as inhaled epinephrine, have similar efficacy to SABAs.[105] They are however not recommended due to concerns regarding excessive cardiac stimulation.[106]
- Long–term control

- Corticosteroids are generally considered the most effective treatment available for long-term control.[99] Inhaled forms such as beclomethasone are usually used except in the case of severe persistent disease, in which oral corticosteroids may be needed.[99] It is usually recommended that inhaled formulations be used once or twice daily, depending on the severity of symptoms.[107]
- Long-acting beta-adrenoceptor agonists (LABA) such as salmeterol and formoterol can improve asthma control, at least in adults, when given in combination with inhaled corticosteroids.[108] In children this benefit is uncertain.[108][109] When used without steroids they increase the risk of severe side-effects[110] and even with corticosteroids they may slightly increase the risk.[111][112]
- Leukotriene antagonists (such as montelukast and zafirlukast) may be used in addition to inhaled corticosteroids, typically also in conjunction with LABA.[99] Evidence is insufficient to support use in acute exacerbations.[113][114] In children under five years of age, they are the preferred add-on therapy after inhaled corticosteroids.[115]
- Mast cell stabilizers (such as cromolyn sodium) are another non-preferred alternative to corticosteroids.[99]
- Delivery methods
- Adverse effects
Others
When asthma is unresponsive to usual medications, other options are available for both emergency management and prevention of flareups. For emergency management other options include:- Oxygen to alleviate hypoxia if saturations fall below 92%.[119]
- Magnesium sulfate intravenous treatment has been shown to provide a bronchodilating effect when used in addition to other treatment in severe acute asthma attacks.[10][120]
- Heliox, a mixture of helium and oxygen, may also be considered in severe unresponsive cases.[10]
- Intravenous salbutamol is not supported by available evidence and is thus used only in extreme cases.[119]
- Methylxanthines (such as theophylline) were once widely used, but do not add significantly to the effects of inhaled beta-agonists.[119] Their use in acute exacerbations is controversial.[121]
- The dissociative anesthetic ketamine is theoretically useful if intubation and mechanical ventilation is needed in people who are approaching respiratory arrest; however, there is no evidence from clinical trials to support this.[122]
Alternative medicine
Many people with asthma, like those with other chronic disorders, use alternative treatments; surveys show that roughly 50% use some form of unconventional therapy.[126][127] There is little data to support the effectiveness of most of these therapies. Evidence is insufficient to support the usage of Vitamin C.[128] Acupuncture is not recommended for the treatment as there is insufficient evidence to support its use.[129][130] Air ionisers show no evidence that they improve asthma symptoms or benefit lung function; this applied equally to positive and negative ion generators.[131]"Manual therapies", including osteopathic, chiropractic, physiotherapeutic and respiratory therapeutic maneuvers, have insufficient evidence to support their use in treating asthma.[132] The Buteyko breathing technique for controlling hyperventilation may result in a reduction in medications use however does not have any effect on lung function.[100] Thus an expert panel felt that evidence was insufficient to support its use.[129]
Prognosis

no data
<100 div="">
100–150
150–200
200–250
250–300
300–350
|
350–400
400–450
450–500
500–550
550–600
>600
|
Epidemiology
Main article: Epidemiology of asthma

no data
<1 div="">
1-2%
2-3%
3-4%
4-5%
5-6%
|
6-7%
7-8%
8-10%
10-12.5%
12.5–15%
>15%
|
While asthma is twice as common in boys as girls,[16] severe asthma occurs at equal rates.[140] In contrast adult women have a higher rate of asthma than men[16] and it is more common in the young than the old.[40]
Global rates of asthma have increased significantly between the 1960s and 2008[141][142] with it being recognized as a major public health problem since the 1970s.[40] Rates of asthma have plateaued in the developed world since the mid-1990s with recent increases primarily in the developing world.[143] Asthma affects approximately 7% of the population of the United States[110] and 5% of people in the United Kingdom.[144] Canada, Australia and New Zealand have rates of about 14–15%.[145]
History

In 1873, one of the first papers in modern medicine on the subject tried to explain the pathophysiology of the disease while one in 1872, concluded that asthma can be cured by rubbing the chest with chloroform liniment.[147][148] Medical treatment in 1880, included the use of intravenous doses of a drug called pilocarpin.[149] In 1886, F.H. Bosworth theorized a connection between asthma and hay fever.[150] Epinephrine was first referred to in the treatment of asthma in 1905.[151] Oral corticosteroids began to be used for this condition in the 1950s while inhaled corticosteroids and selective short acting beta agonist came into wide use in the 1960s.[152][153]
During the 1930s–1950s, asthma was known as one of the "holy seven" psychosomatic illnesses. Its cause was considered to be psychological, with treatment often based on psychoanalysis and other talking cures.[154] As these psychoanalysts interpreted the asthmatic wheeze as the suppressed cry of the child for its mother, they considered the treatment of depression to be especially important for individuals with asthma.
SOURCE: wikipedia











0 comments:
Post a Comment